Using a real clinical case as an example, the experts, Dr Jeroen Dekervel (gastro-oncologist, UZ Leuven) and Dr Roberto Salgado (pathologist, GZA Hospital Networks Antwerp), share their views on how immunotherapy changed the treatment landscape in Upper GI cancers and how to navigate the complexities and controversies of PD-L1 CPS testing associated with the arrival of those new indications.
This website is intended for healthcare professionals based in Belgium and Luxembourg.If you are not a healthcare professional in Ireland, click here
BMS Satellite symposium – February 9, 2022
to address recent developments in advanced Upper GI adenocarcinomas

Upper GI and CPS:
A Ping Pong game between a Pathologist and an Oncologist
With Dr. R. Salgado ZNA-GZA and Prof. J. Dekervel UZ Leuven
BMS Satellite symposium – February 9, 2022
to address recent developments in advanced Upper GI adenocarcinomas
Upper GI and CPS:
A Ping Pong game between a Pathologist and an Oncologist
With Dr. R. Salgado ZNA-GZA and Prof. J. Dekervel UZ Leuven
1
 1:49
1:49
1:49
WHAT IS PD-L1 CPS?
CPS, TPS, IC
2
 02:43
02:43
02:43
CONCORDANCE BETWEEN TESTS: DOES THE ASSAY MATTER?
Interchangeability of assays
3
 00:51
00:51
00:51
CONCORDANCE BETWEEN TESTS: DOES THE ASSAY MATTER
Current reimbursement criteria
4
 02:24
02:24
02:24
WHICH TYPE OF SAMPLE SHOULD BE TESTED PREFERRABLY?
Primary, lymph node or metastasis
5
 01:18
01:18
01:18
WHICH TYPE OF SAMPLE SHOULD BE TESTED PREFERRABLY?
Treated or untreated?
6
 03:01
03:01
03:01
REPORTING CPS: RECOMMENDATIONS TO PATHOLOGISTS?
Reporting CPS & TPS as a continuous variable
7
 26:40
26:40
26:40
FULL VIDEO
1
1:49
1:49
WHAT IS PD-L1 CPS?
CPS, TPS, IC
PD-L1 is an immune biomarker which has emerged as a predictive biomarker of response to immunotherapy notably in Upper GI.1,2
PD-L1 can be expressed both in tumor cells (TC) and in tumor infiltrating immune cells (IC) (video 1).
- CPS : PD-L1 expression can be evaluated in tumor cells only (TPS), immune cells only (IC) or in both compartments (Combined Positivity Score, CPS).
- CPS is the amount of PD-L1 positive tumor cells + the amount of PD-L1 positive lymphocytes and macrophages, divided by the amount of tumor cells.
1. SmPC Opdivo; 2. SmPC Pembrolizumab.
2
02:43
02:43
CONCORDANCE BETWEEN TESTS: DOES THE ASSAY MATTER?
Interchangeability of assays
Dr. Dekervel wonders whether using another assay that the one used in the clinical trials might deliver a different CPS result (video 2).
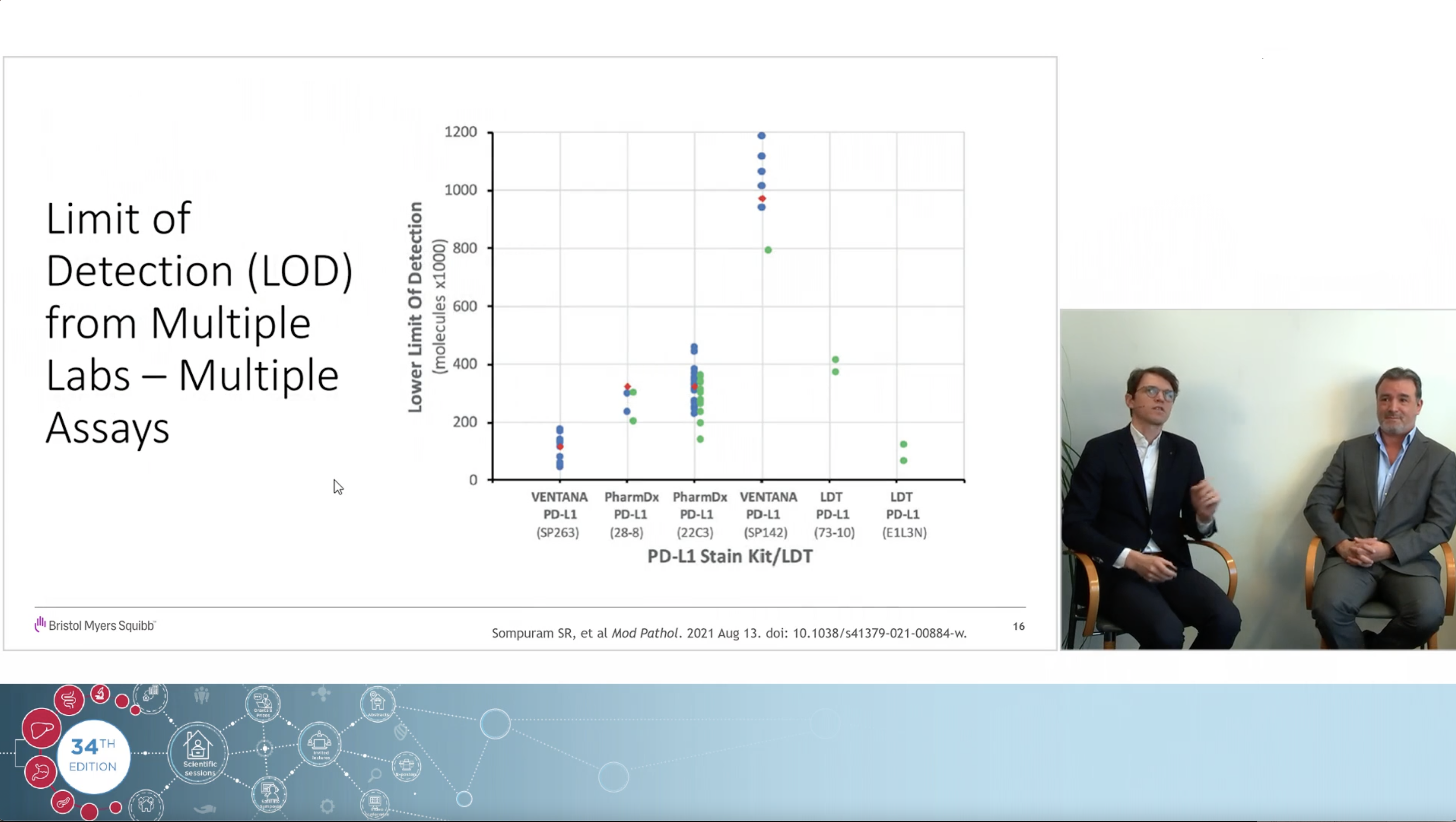
- Dr Salgado thinks that, with some exceptions, most PD-L1 kits have equivalent analytical performance
- Dr Salgado describes two recent studies in various tumor types, showing that most PD-L1 assays have nearly equivalent staining sensitivity.
- Although strictly speaking PD-L1 assays are not interchangeable, the variability between those assays is extremely low; in practice, those various assays will deliver similar results.
- Regarding the 28-8 and 22C3 assays, they are so comparable that it doesn’t matter practically which one is used for determining PD-L1 expression.
3
00:51
00:51
CONCORDANCE BETWEEN TESTS: DOES THE ASSAY MATTER
Current reimbursement criteria
In addition, Dr Dekervel asks whether current reimbursement criteria impose the use of a specific assay to be able to prescribe a specific drug (video 3).
- Dr Salgado says It is not necessary to use a companion diagnostic for prescribing immunotherapy.
- EU label and local reimbursement criteria do not specify the test to be used: any validated PD-L1 assay can be used.
- Laboratory-developed tests (LDT) have equivalent analytical performance to companion diagnostic assays.
4
02:24
02:24
WHICH TYPE OF SAMPLE SHOULD BE TESTED PREFERRABLY?
Primary, lymph node or metastasis
- Since the assay does not matter, does the biopsy site/tissue have an impact?
- Larger amounts of infiltrating immune cells are observed in the lymph node and lungs, and fewer are observed in liver and skin (video 4).
- Cancerous lymph nodes, by default, have more immune cells and PD-L1 positivity.
- What about EUS biopsy ? Dr Salgado does not recommend performing PD-L1 analysis on cytology specimens, because the pathologist needs to evaluate the spatial patterns of the staining on the specimen.
5
01:18
01:18
WHICH TYPE OF SAMPLE SHOULD BE TESTED PREFERRABLY?
Treated or untreated?
- Should one use untreated or treated samples (video 5)?
Immune system goes down after treatment and in metastases vs primary. Chances of revealing CPS are higher in untreated, primary samples. If one has to biopsy metastatic tissue, preferably use lymph node or lung biopsies.
6
03:01
03:01
REPORTING CPS: RECOMMENDATIONS TO PATHOLOGISTS?
Reporting CPS & TPS as a continuous variable
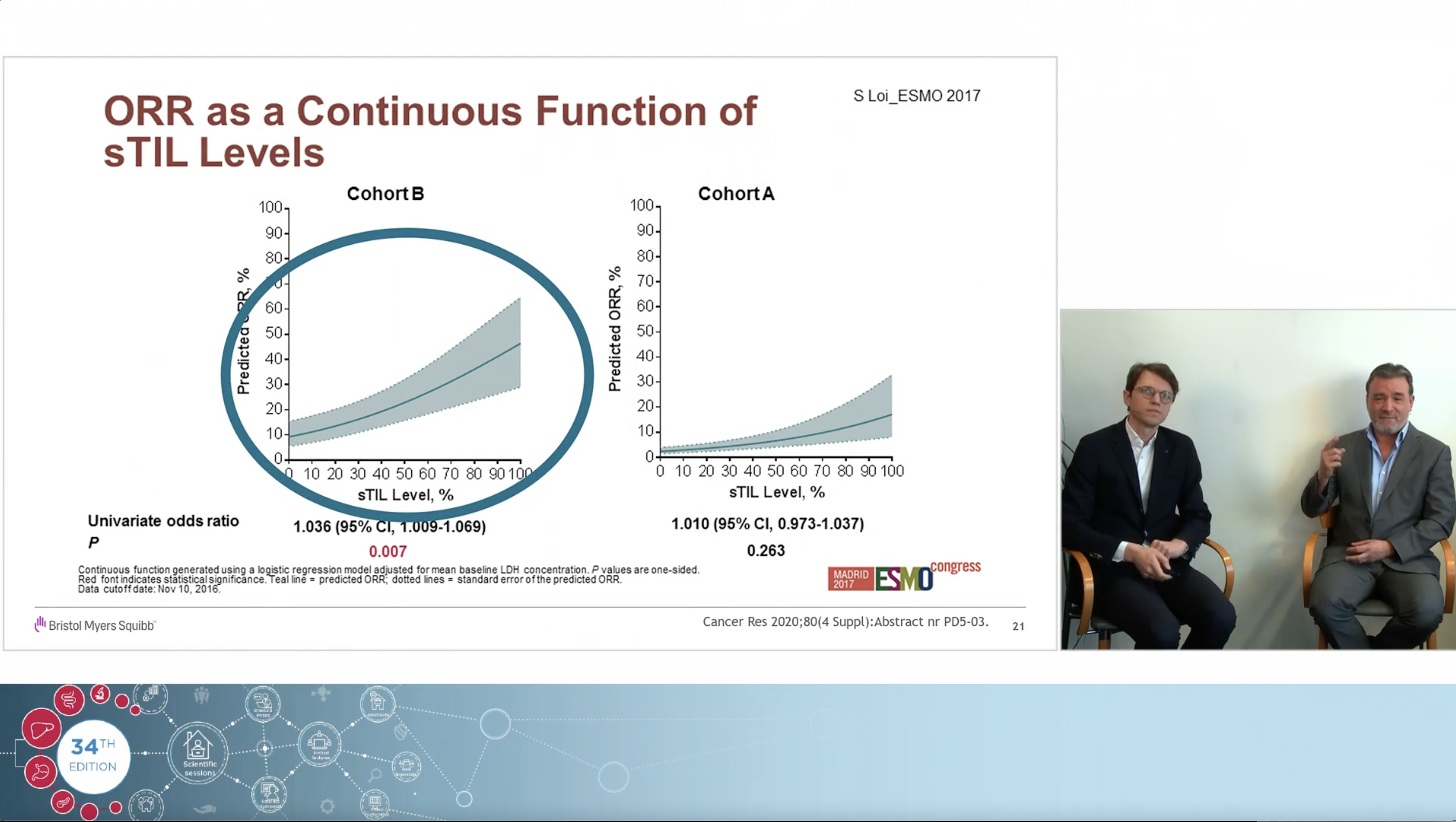
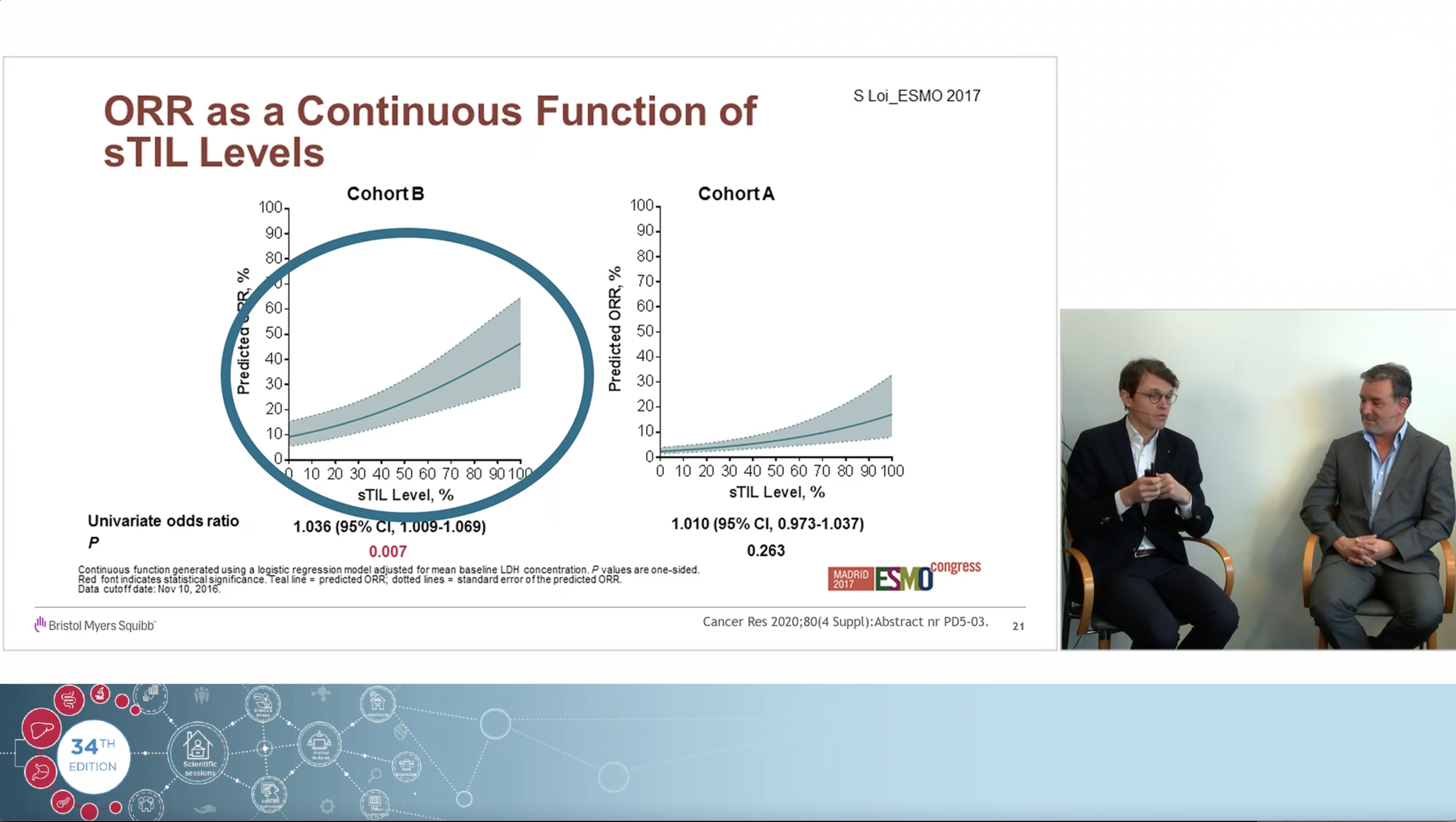
- Reporting CPS as a continuous variable should be preferred over reporting by thresholds. It allows for easier evaluation of patient eligibility for available immunotherapies (i.e. nivolumab or pembrolizumab) (video 6).
- Pathologists should also report values of sub-components of CPS, i.e. tumor cell positivity and immune cell positivity. This will allow easier treatment decision, notably in ESCC where both pembrolizumab (CPS>10) and nivolumab (TPS>1%) are reimbursed in Belgium.
7
26:40
26:40
FULL VIDEO
1506-BE-2200032 – 05/2022
You may contact our EU Data Protection Officer at EUDPO@BMS.com to exercise any data privacy rights that you may have, as well as to raise any concerns or questions in relation to the handling of your personal data by Bristol-Myers Squibb Company.